I know that I’ve said it before, but I really do miss the old days, the days before President Donald Trump nominated Robert F. Kennedy Jr., a man who’s been a rabid antivax activist for the last 20 years to be Secretary of Health and Human Services (HHS), a position that put him in charge of all non-military programs in healthcare, medicine, biomedical research, and public health. This includes the Food and Drug Administration (now lead by FDA Commissioner and COVID-19 contrarian Dr. Marty Makary), the Centers for Disease Control and Prevention (not currently led by anyone yet, and thus apparently being run by RFK Jr. for now), the National Institutes of Health (led by COVID-19 “natural herd immunity” maven and Great Barrington Declaration co-author now bent on revenge against his perceived enemies for his pandemic era “cancellation” and “persecution”), and the Centers for Medicare and Medicaid Services (now led by America’s Quack, Dr. Mehmet Oz). Back then, I could write posts about homeopathy, run-of-the-mill cancer quackery, misunderstood issues in medicine like overdiagnosis, and sometimes just fun basic science. Since late last year, and especially since early this year, when the entire federal health establishment was co-opted by antivaxxers, quacks, and grifters, who are systematically destroying the public health infrastructure of the US, it seems that whenever Monday (and my turn to post here) rolls around, it’s back to RFK Jr. and the current administration.
So it was two weeks ago, when I wrote about how RFK Jr. had purged all 17 members of the Advisory Committee on Immunization Practices (ACIP), the committee responsible for determining which vaccines are included in the CDC recommended immunization schedule and replaced them with a mix of antivaxxers, the antivax-curious or -adjacent, and the incompetent, I knew that I’d soon have to write about ACIP again, and so it came to pass last week, when I described how I thought ACIP would begin dismantling the US federal vaccination system. Of course, the first meeting of the reconstituted ACIP was held last Wednesday and Thursday; so I knew I’d have to make my series on ACIP into a trilogy of terror, if you will, because how could I write so much about the lead up without actually describing what happened? Fortunately for my blood pressure, work on Wednesday and Thursday kept me away from my office, where I might have been tempted to listen to the entire thing live, which might have led me to pulling out the little hair that I have left. I have, however, listened to parts of it at my own leisure, statements about it, as well as what some others have written about it.
The clown car disgorges its clowns to start the meeting
As I was preparing to write about this, I can’t help but just say that a certain Seattle cartoonist named David Horsey got it disturbingly right:
On the other hand, my analogy of the clown car might be better, because one of the dominant impressions I got from last week’s ACIP meeting was one of overwhelming incompetence, even despite the best efforts of career CDC staff to keep things in line. A couple of incidents reinforcing that impression occurred even before the meeting started. First, one of the eight members appointed by RFK Jr., Dr. Michael Ross, resigned. The reasons are unclear. Some stories suggested that it was because of the rigorous financial vetting for conflicts of interest, and even the HHS statement seemed to suggest that this was the case:
“Dr. Michael Ross decided to withdraw from ACIP during the financial holdings review required of members before they can start work on the committee,” an HHS spokesperson told Fierce Pharma.
“The sacrifice to serve on ACIP varies from member to member, and we appreciate Dr. Ross’s willingness to go through this rigorous process,” he said, adding that the panel would have benefited from Ross’ service and expertise.
Ross, who previously served on the CDC’s Advisory Committee for the Prevention of Breast and Cervical Cancer, is no longer listed among the voting ACIP members on the CDC’s website.
Elsewhere, it was suggested that there might have been other reasons:
Some experts said they were unsurprised to hear that Dr. Ross was leaving the panel.
“Given the H.H.S. interference into the A.C.I.P. process and meeting agenda, it’s no surprise to me that even members of this R.F.K. hand-selected committee would not feel comfortable participating in such an orchestrated event that bypasses scientific evidence and transparency,” said Dr. Lakshmi Panagiotakopoulos, who resigned from the C.D.C. this month.
Personally, I’m betting that it was the financial vetting for COIs. After all, if you say yes to an offer from RFK Jr. to serve on his reconstituted ACIP, you know that you’re going to be sitting on a committee with antivaxxers designed to come to pre-ordained conclusions about vaccines not based on science. That comes with the territory, and if you weren’t aware of that you deserve all the humiliation that you will endure.
The second incident that contributed to the amateur hour flavor of this meeting came when apparently Dr. Robert “inventor of mRNA vaccines” Malone, a scientist who had made early contributions to liposomally-delivered mRNA molecules as vectors to express proteins, including as vaccines, but then, due to jealousy and feeling overlooked, touted himself as The One True Inventor of mRNA Vaccines, even as he himself turned into a rabid antivaxxers, appeared not to have known before RFK Jr. announced that he had been appointed as co-chair of the committee. Actually, it’s unclear whether Malone knew before RFK Jr. announced that Martin Kulldorff would chair the committee and that Malone would be co-chair that he was to be co-chair. It probably doesn’t matter. Whatever the case, the reporting just the day before the meeting of who would be the co-chairs did not contribute to an impression that this meeting would be well-organized. How could it be, when the entire old committee had been purged a mere two weeks before the meeting in favor of eight new members, all of whom had little or no experience with such an undertaking.
In any event, “clown car” is a good metaphor for this meeting. So is my quip that the antivaxxers in ACIP were partying like it’s 1999, mainly because, as I described last week, they planned to bring up the topic of thimerosal-containing influenza vaccines and what recommendations to make about them. (It was decided in 1999 to remove the mercury-containing preservative thimerosal from childhood vaccines, a process that was complete no later than 2002, but thimerosal could still be used as a preservative in multidose vials. Few flu vaccines are in multidose vials anymore.) The issue of thimerosal-containing flu vaccines is as good a place as any to start, in order to illustrate how science was twisted and misrepresented to promote an antivax agenda, even if the end result of this meeting, at least, was not as horrific as it might have been.
I don’t plan on discussing every aspect of the meeting, but rather to take more of an overview. However, one incident must be considered, and that’s how the committee handled the question of thimerosal-containing flu vaccines.
Partying like it’s 1999…sort of
Back in the early days of my activities writing about quackery and the antivax movement, I liked to point out that, c.1998-2006 or so, there were two main branches—factions if you will—of the antivax movement. First, of course, there was the mainly British contingent that blamed the MMR vaccine for autism, spurred on by Andrew Wakefield’s fraudulent 1998 case series published in The Lancet. The other contingent is one that I (and others) used to like to refer to derisively as the “mercury militia.” They believed fervently that mercury in the thimerosal preservative that had been used in a number of childhood vaccines was actually The One True Cause of Autism. Indeed, RFK Jr. came out of the mercury militia side of the antivax movement, and his “coming out article” Deadly Immunity in 2005 posited a conspiracy theory in which the CDC supposedly “knew” that thimerosal-containing vaccines caused autism but had met in 2000 at the Simpsonwood Conference Center in suburban Atlanta to “cover up” the “inconvenient data” supposedly showing the link, which is why I call this particular conspiracy theory the Simpsonwood conspiracy theory.
A quarter century on, claim that thimerosal in vaccines was the main “environmental exposure” causing an “autism epidemic” is fairly easy to debunk, mainly because, as I mentioned above, thimerosal was ordered removed from childhood vaccines in 1999 a process completed by 2002. If thimerosal-containing vaccines were indeed a major cause of autism, one would expect that the removal of thimerosal from childhood vaccines would result in a decrease in autism prevalence that would be detectable a few years after the removal. Guess what didn’t happen? That’s right, autism prevalence did not decline; rather, it continued its upward trajectory, a trajectory that didn’t even detectably slow. That, taken in the context of the copious other evidence that vaccines, thimerosal-containing or not, don’t cause autism, made for a very compelling natural experiment that resoundingly falsified the hypothesis that thimerosal-containing vaccines were a major cause of autism. Its’ why, since 2008, I have referred to this hypothesis as a failed hypothesis.
Indeed, so failed was the thimerosal-autism hypothesis that RFK Jr.’s original antivax group, the World Mercury Project, eventually conceded reality and rebranded itself as Children’s Health Defense, its current name. Similarly, Generation Rescue, an antivax group founded by J.B. Handley and his wife (and for a while fronted by Jenny McCarthy), was based on the idea that mercury in vaccines caused autism but eventually forced to broaden its antivax message to embrace other fantastical mechanisms by which antivaxxers thought vaccines could cause autism and downplay mercury. All of this history is why I did a double-take when I first read that the new ACIP meeting would be examining the question of whether it continues to recommend thimerosal-containing flu vaccines, which are mainly given to adults and seldom to children, meaning that autism was not even a consideration.
At this point, it’s also worth comparing and contrasting how ACIP has traditionally been run with how this meeting of ACIP was run. In general, scientific questions with respect to vaccines don’t make it to a full ACIP meeting until after various working groups associated with ACIP have spent months or even years looking at the scientific evidence, synthesizing it, and then writing a report and presentation for the full committee to consider prior to voting on a recommendation. Say what you will about it, but it was a rigorous process, aided by career CDC scientists. Indeed, the whole process is supposed to use what is called an Evidence to Recommendations (EtR) framework that looks at multiple domains. Take a look at the link I just listed, which will lead you to a CDC document with the framework and the domains to be considered, which include:
- Is the problem of public health importance?
- How substantial are the desired anticipated effects?
- How substantial are the undesired anticipated effects?
- Do the desirable effects outweigh the undesirable effects?
- What is the overall certainty of evidence for the critical outcomes?
- Does the target population feel that the desirable effects are large relative to undesirable effects?
- Is there important uncertainty about or variability in how much people value the main outcomes?
- Is the intervention acceptable to key stakeholders?
- Is the intervention a reasonable and efficient allocation of resources?
- What would be the impact on health equity?
- Is the intervention feasible to implement?
At each stage, to consider each question, evidence is supposed to be evaluated according to the GRADE framework, which systematically rates the quality of evidence available to apply to each question above. Indeed, as Ed Nirenberg notes, going through these assessments is what used to take up the majority of time in ACIP meetings. (I particularly like how Ed drolly noted that this “is, in fact, gold standard science,” thus throwing back RFK Jr.’s deceptive MAHA buzzword back into his face.)
In any event, back to the EtR framework. After answering all these questions, ACIP is supposed to come up with a recommendation, which can include:
- ACIP does not recommend the intervention. (Intervention may be used within FDA licensed indications, however.) Or:
- ACIP recommends the intervention for individuals based on shared clinical decision-making, or:
- ACIP recommends the intervention.
Again, although not perfect, this is a rigorous and mostly reproducible framework to come up with clinical recommendations regarding vaccines based on evidence. Indeed, another buzzword besides “gold standard science” at ACIP was “evidence-based medicine.” According to this article in The Atlantic by Daniel Engber, Kulldorff kept repeating the term “evidence-based medicine” like an exorcism to ward off inconvenient criticism of how much the ACIP process had been corrupted:
Throughout the two-day meeting, Kuldorff kept returning to a favorite phrase: evidence-based medicine. “Secretary Kennedy has given this committee a clear mandate to use evidence-based medicine,” he said on Wednesday morning. “The purpose of this committee is to follow evidence-based medicine,” he said on Wednesday afternoon. “What is important is using evidence-based medicine,” he said again when the meeting reached its end. All told, I heard him say evidence-based at least 10 times during the meeting. (To be fair, critics of Kuldorff and his colleagues also love this phrase.) But the committee was erratic in its posture toward the evidence from the very start; it cast doubt on CDC analyses and substituted lay advice and intuition for ACIP’s normal methods of assessing and producing expert consensus. “Decisons were made based on feelings and preferences rather than evidence,” Morris told me after the meeting. “That’s a dangerous way to make public-health policy.”
Oops. I just gave away the answer to the question I was going to ask now: Did ACIP go through all these steps with respect to the question of recommending thimerosal-containing vaccines? I think you know the answer to that:
What did ACIP do instead? They viewed a single presentation by Lyn Redwood, a longtime antivax activist and RFK Jr. buddy affiliated with his antivax group Children’s Health Defense back in the days when it was called the World Mercury Project. You can guess the quality of the presentation. Talk about partying like it’s 1999! Some of the tropes, misinformation, and lies about thimerosal in the presentation were so old that I had forgotten about them, not having had to consider them for at least a decade—or even more. Amusingly, much like the infamous MAHA Report, an early version of the presentation posted to the CDC website appears to have had at least one fake citation that didn’t exist, leading some experts to wonder if the presentation had been written in part by AI, producing AI slop and hallucinations. Moreover, Lyn Redwood has no relevant scientific training or expertise, which led Kulldorff to attack her critics as criticizing her because she doesn’t have a PhD or MD, rather than because she was spewing very old, very discredited pseudoscience.
I debated whether to go through the presentation point by point, but decided against it, given that, thanks to Ed Nirenberg, I know that there’s a TEC brief that does that. However, I will say that, perusing the reference list and the slides, I immediate recognized a lot of old thimerosal-related antivax tropes. Let’s take a look at her summary slides:
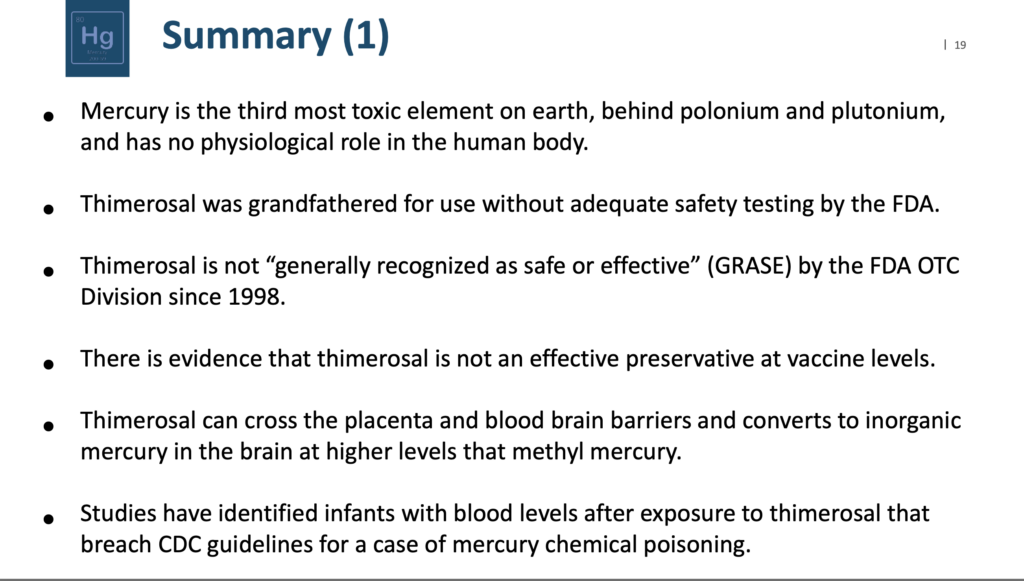

Basically, the presentation cherry picked the usual old antivax studies, many of which were carried out before the pharmacology of ethyl mercury was as well understood as it is now, used in vitro and animal studies while ignoring all the epidemiological studies that failed to find evidence of harm to children from the use of thimerosal-containing vaccines, failed to consider the low dose of thimerosal that is received from vaccines, and often conflated methylmercury, which is a lot more toxic and not eliminated from the body as rapidly as ethyl mercury (thimerosal). None of this is new. It’s what antivaxxers have been doing since the 1990s. Moreover, one just has to point out that thimerosal-containing childhood vaccines other than the flu vaccine were off the market by the end of 2022, but autism prevalence has continued to rise to show how ridiculous this all is. Antivaxxers used ACIP to try to relitigate a scientific question that was settled more than two decades ago and then voted against the use of thimerosal-containing flu vaccines based on no good evidence:
- To reaffirm recommendation, by a vote of six to zero, for routine annual influenza vaccination of all persons aged over six months who do not have contraindications.
- To recommend, by a vote of five to one, for children 18 years and younger to receive seasonal influenza vaccines only in single-dose formulations that are free of thimerosal as a preservative.
- To recommend, by a vote of five to one, that pregnant women receive seasonal influenza vaccines only in single-dose formulations that are free of thimerosal as a preservative.
- To recommend, by a vote of five to one, that all adults receive seasonal influenza vaccines only in single-dose formulations that are free of thimerosal as a preservative.
Who was the one person who did not go along with ACIP? It was Cody Meissner, who has served on ACIP before:
The only one of Kennedy’s appointees who had ever previously served on the committee—the pediatrician Cody Meissner—seemed perplexed, even pained, by the proceedings. “I’m not quite sure how to respond to this presentation,” he said when Redwood finished. He went on to sum up his concerns: “ACIP makes recommendations based on scientific evidence as much as possible. And there is no scientific evidence that thimerosal has caused a problem.” Alas, Meissner’s warnings were for nought. Throughout the meeting, he came off as the committee’s last remaining, classic “expert”—a vaccine scientist clinging to ACIP’s old ways—but his frequent protestations were often bulldozed over or ignored. In the end, his was the only vote against the resolutions on thimerosal.
To this I ask Dr. Meissner: WTF did you expect when you agreed to be on ACIP under RFK Jr.? Are you having second thoughts about your life choices when it comes to fraternizing with enemies of public health like RFK Jr.? Inquiring minds want to know!
Emotion-based decision-making
Indeed, not related to thimerosal and returning to the “emotion-based” decision-making, let’s look at monoclonal antibodies against respiratory syncytial virus (RSV), a man whose X account features this pinned post lying about mRNA-based COVID-19 vaccines:
Levi made a name for himself in the COVID-19 antivax crankosphere with some truly bad science linking cardiac death to COVID-19 vaccination. A man with no relevant expertise in epidemiology, infectious disease, vaccines, or public health, he is a former Israel Defense Forces intelligence officer and an academic whose background is in data modeling, risk management, and organizational logistics. Not that that stopped him from some serious Dunning-Kruger and being a highly annoying individual—and not in a good way:
He approached the proceedings with a swaggering incredulity, challenging the staffers’ efforts and pointing out the risks of systematic errors in their thinking. (In a pinned post on his X profile, Levi writes that “the evidence is mounting and indisputable that mRNA vaccines cause serious harm including death”—a position entirely at odds with copious data presented at the meeting.)
Shortly before the committee’s vote to recommend a new, FDA-approved monoclonal antibody for preventing RSV in infants, Levi noted that he’d spent some time reviewing the relevant clinical-trial data for the drug and another like it, and found some worrying patterns in the statistics surrounding infant deaths. “Should we not be concerned that maybe there are some potential safety signals?” he asked. But these very data had already been reviewed, at great length, in multiple settings: by the FDA, in the course of drug approval, and by the dozens of members of ACIP’s relevant work group for RSV, which had, per the committee’s standard practice, conducted its own staged analysis of the new treatment before the meeting and reached consensus that its benefits outweighed its risks. Levi was uncowed by any reference to this prior work. “I’m a scientist, but I’m also a father of six kids,” he told the group; speaking as a father, he said, he personally would be concerned about the risk of harm from this new antibody for RSV.
In the end, Levi voted against recommending the antibody, as did Vicky Pebsworth, who is on the board of an anti-vaccine organization and holds a Ph.D. in public health and nursing. The five other members voted yes.
In other words words, even though real experts had done a staged EtR framework analysis, real “gold standard science,” if you will, Levi thought that his anecdotal feels trump science. Indeed, one can’t help but refer to what Martin Kulldorff said in response to a question about the EtR process and how it wasn’t being followed. Basically, he defended Lyn Redwood as being “very knowledgeable about vaccines.” Sure, sort of, the same way that Alex Jones is “very knowledgeable” about 9/11, Sandy Hook, and chemtrails.
Meanwhile, the contrast between the utter lack of qualifications and content knowledge of all but one ACIP member could not have been more stark in comparison to the science, professionalism, and cool of the CDC career scientists given the unpleasant task of presenting actual vaccine science to the ACIP clown car. They tried to present the actual science of COVID-19 vaccines and directly contradicted RFK Jr.:
CDC studies found “no increased risk” that the Moderna and Pfizer mRNA vaccines caused adverse effects during pregnancy, Sarah Meyer, director of the CDC’s Immunization Safety Office, said at the meeting, citing data from 28 analyses of 68,000 pregnant women. The data showed no increases in miscarriages, stillbirths, preterm births, major birth defects, neonatal ICU admissions, infant deaths, abnormal uterine bleeding or other pregnancy-related conditions.
In fact, the CDC found that “maternal vaccination is the best protection against COVID-19 for pregnant women and infants less than six months of age,” CDC immunologist Adam MacNeil told the panel. The COVID vaccines aren’t approved for infants younger than six months, so maternal immunization is their only protection.
That’s important because Kennedy, on May 17, removed the vaccines from the recommended list for pregnant women and children. “It’s common sense and it’s good science” to remove the recommendation, Kennedy said in a 58-second video posted on X.
Nice going, CDC scientists! Sadly, I fear that you might not be long for your jobs, but I know you know that and salute you for saying a big “Screw you!” to the enemies of public health in charge. You, at least, kept your integrity, whatever the consequences of your speaking truth to power might be.
It was also amusing to see them showing the committee, in including Retsef Levi to his face, how the evidence is overwhelming that COVID-19 vaccines saved millions of lives and were associated with very little harm. He definitely showed that he has little understanding of the epidemiological studies presented, mainly through his questions about “confounders” that were not:
Committee member Dr. Retsef Levi, a professor of operations management at Massachusetts Institute of Technology, asked about potential confounding in the CDC’s studies, which he thought might be showing the opposite conclusions of what the scientists were presenting on efficacy of the current Covid-19 vaccines. He speculated that the control groups of the studies, which consisted of people who had other kinds of respiratory infections, were actually people damaged by Covid-19 vaccinations that put them at greater risk for those respiratory infections.
“In that case, you will assume that the vaccine is protective,” Levi said, “but an alternative explanation would be that the vaccine is actually making you more vulnerable for multiple viruses.”
Dr. Ruth Link-Gelles, a CDC epidemiologist, said that control subjects were chosen to closely match the hospitalized patients with Covid-19 in terms of age and symptoms.
“We think that the controls here are exactly what we want to understand the relative impact of the vaccination,” she said.
Meanwhile, Tracy Beth Høeg was also concerned about “confounders” and wanted randomized controlled clinical trials, again ignoring bioethics and weaponizing evidence-based medicine the way that COVID-19 contrarians have been doing since the pandemic.
The proceedings were followed by a truly delusional press release from ACIP:
Honesty, transparency, and compassion with regard to public health. These are the three pillars that we, the new ACIP members, are guided by. Our central duty is to protect public health, and we understand that we must answer the call for reestablishing confidence in the scientific examination process. This committee strongly supports the use of vaccines, and other countermeasures, predicated on evidence-based medicine, including rigorous evaluation and expansive, credible scientific data, for both safety and efficacy.
All stakeholders, including health care providers, parents, children, schools, nursing homes, insurance providers, public health agencies, manufacturers, and the rare few who may be harmed by recommended interventions, need to have understandable, digestible, scientifically correct information. This group is committed to providing that information, and in order to do so, we must have data representing large populations. Data collection is a central question that may require constructing a broad risk-benefit analysis. The committee will endeavor to assess the status of programs that are intended to collect data from large populations that have, or have not, received vaccines. These data are needed in order to assess both adverse short- and long-term side effects and to evaluate the magnitude of side effects.
We came to this meeting with no pre-determined ideas and will make judgements as if we are treating our own families. Unbiased scientific thinking is fundamental to the committee’s charge. Our votes are recommendations, but we know that some may perceive them as mandates, so we take this responsibility very seriously. We pledge not to hold a vote if there is not sufficient information to enable evaluation of the risks and benefits.
This committee is not in competition with other committees, organizations, or each other – we are all in competition with the infectious diseases, and we will work together to ensure the best outcomes for public health.
They came to the meeting with “no predetermined ideas”? Their votes on thimerosal and their inclusion of Lyn Redwood as sole speaker on the topic suggest otherwise. So does the fact that the CDC scientists’ brief on thimerosal in vaccines, which listed the actual science showing that the additive was not associated with harm and had been posted prior to the start of the meeting, was taken down:
On Thursday, when asked whether the CDC thimerosal document could be reposted, one of the committee members, Dr. Robert Malone, said “my understanding is that article was not authorized by the office of the secretary and has been removed consequent.” Dr. Martin Kulldorff, the chair of the committee, said members had received the briefing document.
Sure, Bob. Anything you say.
ACIP is, at best, unreliable and, at worst, now firmly antivaccine
The whole spectacle that this ACIP meeting provided was deeply depressing. On the one hand, I was half-tempted to say that, when it comes to thimerosal in multidose flu vaccines, maybe that’s not a hill worth dying on, given that only around 5% of flu vaccines are packaged in multidose vials and that ACIP didn’t remove their general recommendations that adults and children receive the flu vaccine…this time, anyway. But then I thought about it some more and realized that this is an intentional tactic on the part of RFK Jr. and his antivax cronies, to cast doubt on all vaccines by relitigating an old antivax trope. Moreover, who is most harmed by getting rid of multidose vaccines? It will be the poor and those in low resource areas. Moreover, once the precedent of an ACIP decision to remove a recommendation for a vaccine based on bad science, no science, and/or pseudoscience has been made, what’s to stop ACIP from doing the same thing with other vaccines?
Nothing.
In fact, it’s worse than that. As part of its effort to destroy our vaccine programs, ACIP announced:
At the start of today’s meeting, ACIP’s new chair, Martin Kulldorff, PhD, a statistician and epidemiologist formerly at Harvard University, announced that there will be changes to the membership of the CDC’s 11 different vaccine working groups and that two more working groups will be added. Both are boilerplate topics of vaccine critics.
One group will evaluate the cumulative effects of vaccines on the CDC’s recommended schedule for children and adolescents. The other will examine vaccines that have been in use for more than 7 years, which will likely include hepatitis B vaccination at birth and the use of MMRV vaccine in young children.
The AAP on X today quickly pushed back on plans to reconsider hepatitis B vaccination for newborns, saying that passing the virus from parent to baby at birth can be deadly. “It is unscientific & dangerous to ignore the success of U.S. vaccination programs or argue that the U.S. should not vaccinate babies for hepatitis B at birth.”
That bit about examining the “cumulative effects of vaccines” on children is nothing more than an antivax trope that Jenny McCarthy used to parrot c.2007-2008 about “too many too soon.” The false idea is that children receive too many vaccines too soon and it somehow harms their immune system; there is no good evidence to support this idea.
As for the birth dose of the hepatitis B vaccine, that’s long been an antivax bogeyman, likely because of the association of hepatitis B with sexual transmission, the same reason that the HPV vaccine receives such hate from antivaxxers. However, as I’ve discussed before and as summarized here, there are quite valid scientific and epidemiological reasons in this country to chose a birth dose of the hepatitis B vaccine, and there is no evidence that the vaccine harms children the way that antivaxxers claim.
So what will these working groups find? Spoiler alert, just as David Geier will undoubtedly find that vaccines cause autism, these working groups will find that too many vaccines too soon harm children (and cause autism) and that the hepatitis B and MMRV vaccines harm children. Just wait. Given who will likely be assigned to these working groups and how they will go about their business, it’s preordained what they will decide.
I will conclude, as is my habit when writing about RFK Jr. and the antivax grifters, quacks, and ideologues who are now in control of our public health apparatus, by warning everyone again never to underestimate RFK Jr.’s desire to eliminate all vaccines or, failing that, to eliminate as much access to vaccines as he can. That is his endgame. That has always been his endgame. He has been rabidly antivax for two decades, at least, and appears to really believe that vaccines do far more harm than good. Worse, he has shown himself to be utterly impervious to and unpersuadable by evidence. ACIP is now just one of his tools to achieve this end; no doubt he’ll cast his eyes on VRBPAC, the FDA committee that decides which vaccines are approved for sale and use in the US.
I think that our ossified medical societies are finally waking up to the danger, after having (mostly) assiduously keeping their heads down and hoping it will all blow over and everything will be fine again. it won’t. For example, a number of medical societies that normally sent liaisons to ACIP meetings have decided to cease to do so, including the American Academy of Pediatrics, IDSA, SHEA, and SAHM. The AAP went beyond that when its president Dr. Susan Kressly announced on YouTube that the AAP will continue publishing its own recommended pediatric vaccination schedule, noting that ACIP “is no longer a credible process” and adding, “We won’t lend our name or our expertise to a system that is being politicized at the expense of children’s health”:
Meanwhile, the Center for Infectious Disease Research and Policy (CIDRAP) at the University of Minnesota in Minneapolis is looking into the creation of a vaccine committee to replace the current corrupted version of ACIP.
Can these non-government entities succeed in countering the now-antivax ACIP? Who knows? We have to try, as the alternative is just to surrender and accept that by 2029 there will likely be many fewer vaccines recommended and paid for, given that ACIP recommendations mandate insurance coverage, and that is an unacceptable outcome. Letting the clowns in the clown car that ACIP has now become dictate public health is an outcome that must be resisted; that is, unless we want to become clowns too.


{kind=link}